When it comes to therapy, detailed and accurate documentation is not just a legal requirement; it’s a fundamental part of ensuring that your clients get the best possible care.
Session notes are where you document your client’s progress, treatment goals, and any significant events that transpire during a session. These notes not only serve as a record for future sessions, but they also provide evidence of treatment effectiveness, making them critical for insurance claims, legal matters, and overall treatment planning.
However, documenting session notes efficiently can be a daunting task. This is where session note templates come in handy. By using structured templates, you can ensure that you’re capturing all the necessary details in a consistent, timely, and accurate manner.
What if a simple template could save you time and stress, allowing you to focus more on your clients and less on paperwork? In this blog, we’ll explore why session notes are essential, break down the key components that every session note should include, and provide you with some practical tips and examples to improve your documentation.
Why are Session Notes Important?
Session notes aren’t just for your benefit; they also serve as a critical tool for your clients, payors, and other healthcare professionals. Here’s why you should prioritize them:
- Documenting your client’s progress: Detailed notes allow you to track development over time, spot patterns in treatment, and adjust and modify your approach when necessary.
- Ensuring reimbursement: Insurance companies rely on comprehensive session notes to approve treatment claims. Without accurate documentation, you risk delayed payments or claim rejections.
- Protecting your practice: In the event of legal scrutiny, well-documented notes provide a safeguard for your clinical decisions and interactions.
While handwritten notes are still prevalent in some practices, technology is making it easier than ever to create, store, and manage your session notes in a digital format. Using session note templates primarily through practice management software like Simply.Coach can keep you organized with their impressive and comprehensive note-taking feature that keeps all your session’s notes in one place while ensuring that you follow all required guidelines and are secured against any possible scrutiny.
Main Components of Session Notes Templates
The structure of your session notes templates is vital to ensure you’re documenting everything required, from your client’s information to their treatment outcomes. Here’s a breakdown of what should be included in each session note template:
1. Basic patient/client and provider information
Every session note template starts with basic details. This is essential to identify that your client and you are involved in the session. Ensure this section includes the following:
- Client name and date of birth
- Session date and time (duration)
- Therapist’s name and credentials
- Client’s insurance information (if applicable)
These details help create an accurate record and confirm that your notes are linked to the correct client for billing, tracking progress, and legal purposes.
2. Narrative summary of the session
A narrative summary of the session is where you capture the main content of the discussion. This section should include:
- Session focus: What was the primary topic or goal of today’s session? Did you work on a specific issue like anxiety, depression, or relationship challenges?
- Progress made: Reflect on the client’s progress or setbacks since the previous session. Were any goals achieved? What interventions or therapeutic techniques were used?
- Client’s emotional state: Document the client’s mood and any significant emotions observed during the session (e.g., distress, relief, frustration).
You must maintain a measurable and objective language throughout this process. For instance, instead of saying, “the client was feeling better,” say, “the client reported a 40% reduction in anxiety symptoms based on a self-reported scale from 1-10.” This breeds clarity and accountability in your session note templates.
3. Key components required by insurance payors
Insurance companies have specific guidelines for what needs to be included in your session notes templates, especially for therapy practices like yours. Be sure to include the following:
- Diagnosis and treatment plan: Make sure to reference your client’s diagnosis (e.g., Generalized Anxiety Disorder) and how the current session aligns with their treatment plan.
- Interventions and methods: List the therapeutic interventions used (e.g., Cognitive Behavioral Therapy, EMDR, MBSR, etc.).
- Progress toward treatment goals: Did the current session contribute to meeting established treatment goals for your client? If so, how?
Including these details tick marks the fact that your notes are compliant and can be used for insurance reimbursements.
Note Template Format and Examples
When it comes to session note templates, structure and consistency are key. Having a standardized template not only helps save time but also allows you to assure the fact that all the necessary information is captured accurately, reducing the risk of errors or omissions.
As digitization is expanding, therapists like you, too, have access to a wide variety of note formats and templates.
There are several types of session note template formats commonly used in therapeutic settings. Let’s take a look at some of the most popular formats and their benefits for you:
1. DAP (Data, Assessment, Plan)
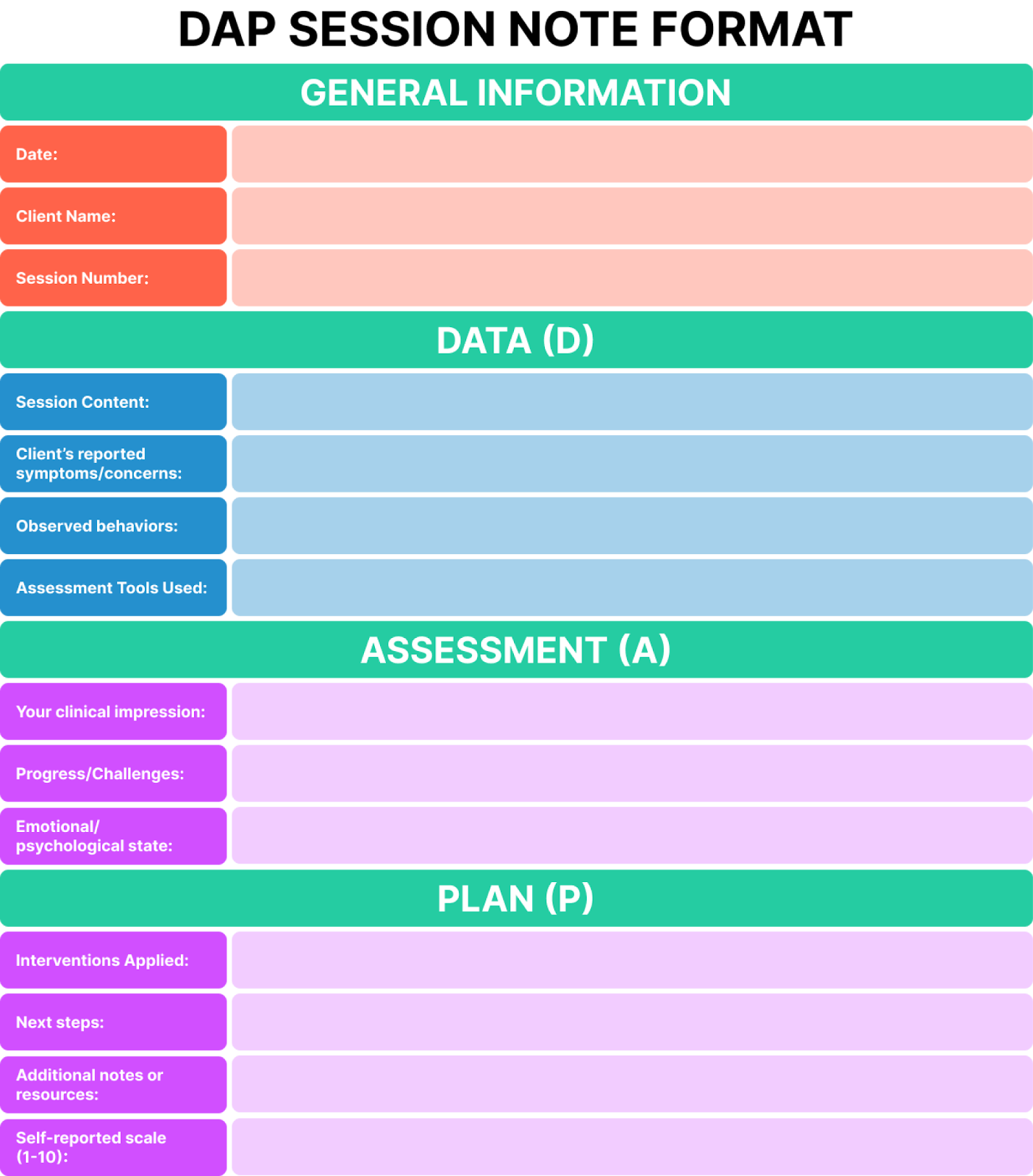
The DAP format is a structured approach that provides clarity and focus to your session notes. It begins with a Data of what occurred during the session, including any observations or events. The Assessment section follows, where you evaluate the client’s progress or challenges, including any changes in their behavior or emotions. The last part is the Plan, where you outline the goals and steps for future sessions. This method is often favored for its simplicity and directness, making it easy to use across a range of therapy practices.
2. BIRP (Behavior, Intervention, Response, Plan)
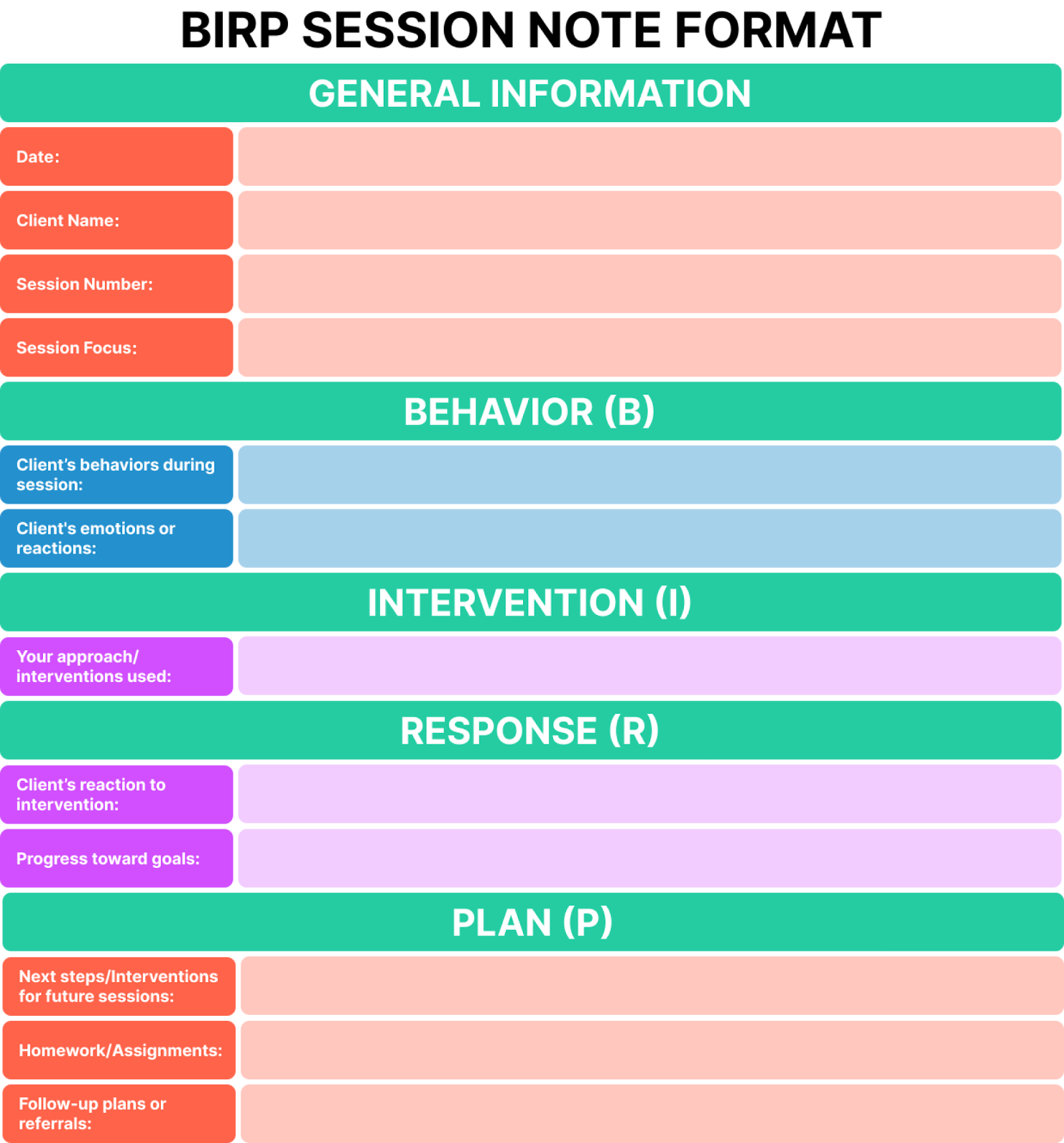
The BIRP format is ideal for behavioral therapy as it provides a clear structure for documenting observable actions. It starts with Behavior, where you record the behaviors that the client displayed during the session. Next, you include the Intervention you used, whether a specific therapeutic technique or approach. In the Response section, you document how the client reacted to the intervention. Finally, the Plan outlines the next steps and the therapeutic goals moving forward. BIRP is particularly useful in cases where tracking specific behaviors is key to progress.
3. SOAP (Subjective, Objective, Assessment, Plan)
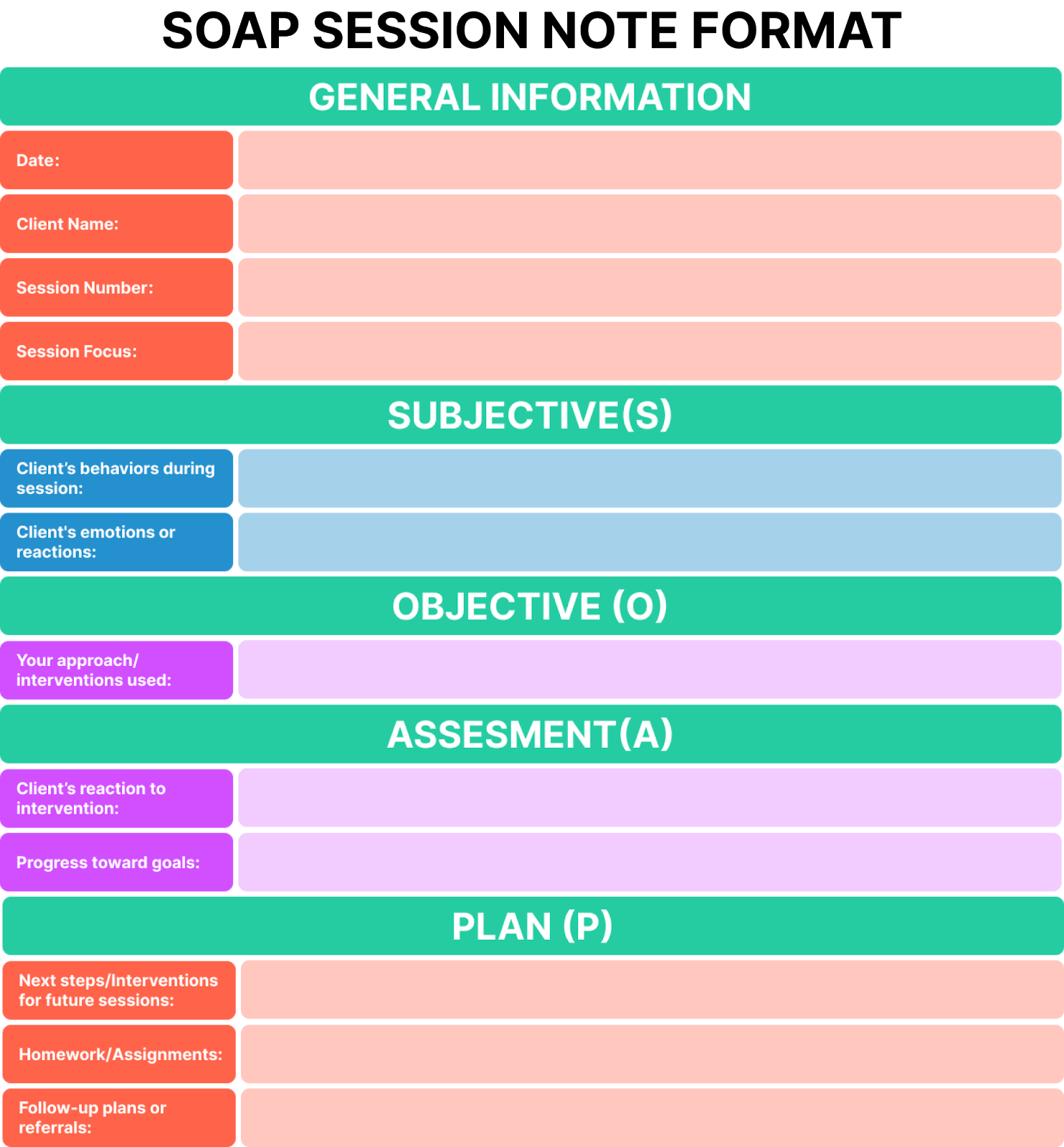
SOAP notes are one of the most widely used formats in therapeutic settings. They begin with the Subjective section, where you capture the client’s personal input or feelings about their condition or progress, usually in their own words. Objective follows, where you note your observations or measurable data, such as test results or physical responses. In the Assessment, you analyze the information and provide your clinical interpretation. Finally, the Plan section outlines the course of action, detailing interventions, goals, and the treatment approach. SOAP is versatile and can be adapted to most types of therapy.
4. GIRP (Goal, Intervention, Response, Plan)
The GIRP format focuses on the therapeutic Goal for the session, which is usually tied to the client’s overall treatment plan. The Intervention section describes the techniques or approaches used to address the goal. Following this, you note the client’s Response to the intervention—was there improvement, resistance, or a change in behavior? Finally, the Plan section focuses on the next steps, including adjustments to the treatment approach or new goals for the client. GIRP is a great template when working with clients on specific, measurable goals.
5. PIRP (Problem, Intervention, Response, Plan)
The PIRP format is quite similar to GIRP but emphasizes the Problem the client is facing before jumping into interventions. After identifying the problem, you proceed with documenting the Intervention employed to address the issue. The Response section notes how the client reacted to the intervention, and the Plan section provides the next steps for therapy. PIRP is useful if you prefer to focus more heavily on understanding the client’s primary issues and adapting treatment accordingly.
6. RIFT (Reason, Intervention, Feedback, Therapy Goals)
RIFT notes start with the Reason for the session, which might include why the client has come in or a specific issue they wish to address. Then, you document the Intervention applied during the session. Feedback follows, where both you and the client provide your inputs on the session’s effectiveness, and Therapy Goals outline the ongoing targets for therapy. This format can be particularly useful for therapists who want to maintain a reflective approach, considering both you and your client’s perspectives on progress.
7. CARE (Client, Assessment, Response, Evaluation)
CARE notes begin by profiling the Client, including relevant background information such as history or specific treatment needs. The Assessment section evaluates the client’s condition and progress, often including any clinical impressions or diagnosis. Response records how the client engaged with the session—did they actively participate, were they resistant, or did they show improvement? Finally, the Evaluation provides an overall review of the client’s progress and any changes in treatment direction. CARE is beneficial for cases where thorough background information and evaluation are essential.
8. STOP (Summary, Treatment, Observation, Plan)
STOP notes provide a brief yet comprehensive record of the session. The Summary section offers a high-level overview of the client’s current condition or presenting issue. In the Treatment part, you document the interventions applied during the session. The Observation section highlights key insights or changes observed in the client’s behavior, mood, or response to therapy. Finally, the Plan focuses on outlining the steps for future treatment, whether immediate next steps or long-term objectives. This format is particularly effective for concise documentation, ideal for sessions that may not require extensive notes.
9. MINT (Motivation, Issues, Next Steps, Therapeutic Tools)
The MINT format centers on understanding the Motivation behind the client’s need for therapy, focusing on what drives them to engage in treatment. Issues section outlines the current challenges the client is facing. The Next Steps section details the plans for moving forward, including any adjustments to treatment strategies. Finally, the Therapeutic Tools section lists any specific techniques or tools you will use in the coming sessions to address the client’s issues. This format is especially helpful for motivation-driven therapy practices.
10. FORT (Focus, Outcome, Response, Tactics)
FORT notes are designed to keep you Focused on the core objectives of the session. The Outcome section records the desired results of the session, such as achieving specific goals or improving certain behaviors. Response notes how the client engaged with the session and whether they showed progress. Lastly, the Tactics section outlines the strategies or interventions that will be used in future sessions to address the client’s needs. FORT is particularly useful if you are aiming to maintain clarity and focus on specific treatment objectives throughout your sessions.
Tips for Writing Effective Session Notes
Writing effective session notes requires precision and clarity to ensure that your documentation is both accurate and useful. By following a few key strategies, you can create session notes that are clear, actionable, and professional.
1. Use measurable and objective language: Your session notes templates should have information that is as objective as possible. Avoid ambiguous terms like “seemed happy” or “was a bit sad.” Instead, use clear, measurable language such as “client reported feeling 50% less anxious today compared to last session” or “client demonstrated 60% improvement in coping with triggers.”
2. Ensure timely documentation: Filling your templates immediately after your session can make a world of difference. Delaying documentation can lead to forgetfulness, missed details, and reduced accuracy. Set aside time after each session to jot down your templates or use voice-to-text tools for faster information filling.
3. Incorporate professional writing standards: While it’s easy to focus on speed, never compromise on quality. Ensure your templates contain information in a legible, concise, and grammatically correct manner. Stick to professional language and avoid using casual or non-clinical terms and jargon.
4. Highlight client progress consistently: Always include updates on your client’s progress compared to previous sessions. For example, if a client achieved a milestone or demonstrated improved coping mechanisms, document it clearly. This makes it easier to track their journey and adjust treatment plans accordingly.
5. Be concise but comprehensive: Avoid overloading your notes with unnecessary details while ensuring that all essential information is included. Focus on key points that add value to understanding the session’s outcomes and planning next steps.
4 Effective Session Note Templates
Using standardized session note templates can significantly reduce the cognitive load of documentation, making it easier to focus on your client’s progress instead of struggling with formatting or missing key details. Templates ensure consistency across your documentation, helping you streamline the process while maintaining clarity.
Below, we’ll dive into four highly effective session note templates that can help you stay organized and save time, all while capturing essential information in a structured way.
Here are some sample templates for your session notes. These examples will help you understand how to structure your session note templates.
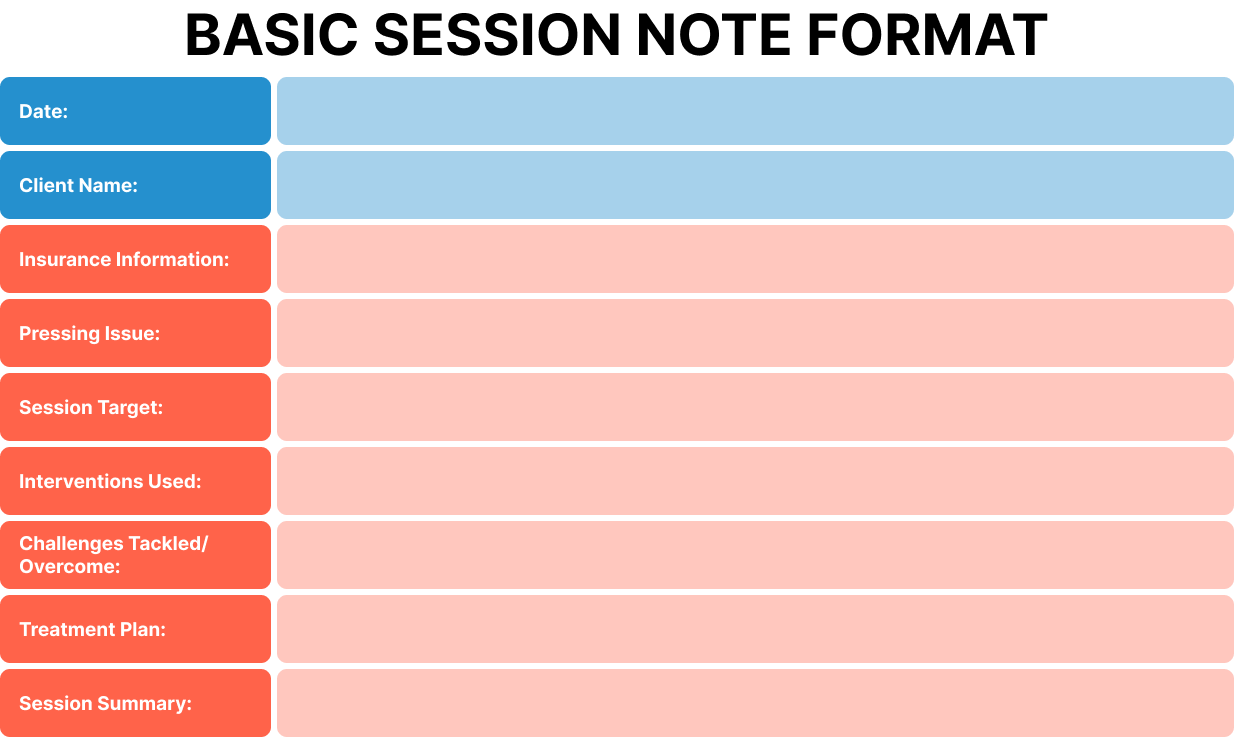
Template 1: Therapy Note Format
Template 2: DAP Session Note Format
Template 3: BIRP Session Note Format
Template 4: SOAP Session Note Format
These examples provide a clear, concise, and structured approach to documenting therapy sessions. By using templates like these, you can streamline the process, ensuring you capture all essential details while saving time.
To further enhance your therapeutic practice, check out our blog post, 50+ Resources, Tools, and Worksheets for Therapists. It’s packed with valuable tools and resources to support your clients’ progress and simplify your work.
Streamline Your Practice with Simply.Coach
Efficient and accurate session documentation is crucial for both legal and clinical purposes, making sure you provide quality care and supporting treatment planning for your clients. Using session note templates simplifies the process for you, serving what you need in a precise, compiled manner, thus reducing stress.
Speaking of collecting compliant session notes, it doesn’t have to be a rigid task. By leveraging the power of automated session notes, the availability of various session note templates, and the right practice management software such as Simply.Coach, you can streamline the process while ensuring HIPAA, SOC2, and GDPR compliance.
With Simply.Coach, you’ll get more than just templates; you’ll gain a comprehensive therapy management tool designed to streamline your workflow, enhance accuracy, and help you focus on what truly matters: your clients.Ready to take your documentation to the next level? Schedule a demo with Simply.Coach or start your 14-day free trial now to experience the benefits firsthand to see how its platform can work for you.
Read More:
7 Best Online Billing Software & Tools for Executive Coaches
The comprehensive client onboarding form template for relationship coaches
Building an Effective Coaching Website: Best Practices and Essentials
Creating On-Brand Coaching Experiences with a Coaching Management System
Effective Marketing Strategies for ADHD Coaches: Reaching and Empowering Individuals with ADHD