You complete a group therapy session with several clients sharing experiences, emotions, and personal challenges. The session feels productive, but the documentation still remains.
Writing clear notes after a group session can feel difficult and time-consuming. You must document each client’s participation while also capturing the overall group discussion.
Many therapists struggle to balance detail and clarity in group therapy documentation. Notes often become repetitive, incomplete, or harder to review during future sessions.
This guide explains how to structure your documentation using practical methods and group therapy notes examples. You will also learn note formats, templates, and simple strategies that make group therapy notes easier to write.
Key Takeaways
- Group therapy notes document both the group process and individual client participation. Therapists must record how each client engages in discussions, responds to peers, and reacts to therapeutic interventions.
- Clear documentation helps track progress and guide treatment planning. Well-written notes reveal behavioral patterns, emotional responses, and changes in participation across multiple sessions.
- Structured note formats improve clarity and consistency. Frameworks like SOAP, DAP, GIRP, and BIRP help therapists organize observations, assessments, interventions, and treatment plans effectively.
- Effective notes focus on observable behaviors and group interactions. Recording how clients speak, respond to peers, and engage in exercises provides meaningful clinical insights.
- Using templates and examples speeds up documentation. Structured templates help therapists write clear notes quickly while maintaining compliance and consistency.
- Practice management platforms like Simply.Coach streamline documentation workflows. Built-in templates, secure client records, and centralized session tracking help therapists maintain organized group therapy notes.
What Are Group Therapy Notes?
Group therapy notes document what happens during a therapy session involving multiple participants. These notes capture the group discussion, therapist interventions, and each client’s level of engagement during the session.
Your notes must reflect how individual clients responded to the group process, not only the topic discussed. Clear documentation helps you track behavioural patterns, emotional reactions, and participation across multiple sessions.
Group therapy notes also record how the group environment influences each client’s progress. Interactions between members often reveal triggers, support patterns, and communication behaviours that individual therapy sessions may not show.
Purpose of group therapy notes in clinical practice
Group therapy notes serve several practical purposes beyond basic record-keeping. They ensure that your sessions produce actionable insights for ongoing treatment.
- Track individual progress within the group setting: Group sessions often involve shared exercises, discussions, and peer feedback. Your notes must show how each client participates, responds to others, and applies therapeutic skills.
- Support treatment planning and goal monitoring: You can review previous notes to evaluate progress toward treatment goals. Documentation helps you adjust interventions when clients show resistance, improvement, or emotional setbacks.
- Maintain clinical accountability: Clear documentation protects your clinical decisions during audits, supervision reviews, and insurance verification processes. Notes must show the therapeutic purpose of the session and your chosen interventions.
- Understand group dynamics over time: Group behaviour often evolves as trust develops between members. Your notes help identify patterns such as dominant participants, withdrawal, peer support, or emerging conflicts.
Also read: How to Write Patient Progress Notes: A Therapist’s Ultimate Guide
Difference between group therapy notes and individual therapy notes
The following table highlights how group therapy documentation differs from individual session notes, focusing on practical clinical distinctions.
| Aspect | Group Therapy Notes | Individual Therapy Notes |
| Session focus | Documents both the group discussion and individual client participation within the shared therapeutic setting. | Focuses entirely on one client’s thoughts, behaviours, and treatment progress. |
| Client interactions | Captures how clients respond to other members, including feedback, conflict, support, and shared experiences. | Client interactions with others are discussed only through the client’s personal perspective. |
| Therapeutic interventions | Records interventions applied to the entire group, such as psychoeducation, group exercises, or structured discussions. | Documents interventions tailored specifically to the individual client’s treatment plan. |
| Behavioral observations | Notes must describe each client’s engagement level, emotional reactions, and communication patterns within the group environment. | Observations focus on the individual client’s mood, behaviour, and responses during the session. |
| Documentation complexity | Requires balancing group-level discussion with individualized client observations in the same session record. | Documentation is simpler because the therapist tracks only one client’s responses and treatment progress. |
| Confidentiality considerations | Notes must avoid identifying details about other group members while still describing interactions accurately. | Confidentiality concerns involve only the individual client. |
Understanding these distinctions helps you decide which details to include for each client, how to summarize group interactions accurately, and how to maintain compliance without overloading your notes.
Also read: Top 9 HIPAA-Compliant Note-Taking Tools for Therapists in 2026 – Simply.Coach
Why Group Therapy Documentation Matters
Group therapy sessions often involve multiple clients sharing complex emotions at the same time. You must track not only individual responses but also how group interactions influence each client. Without detailed records, it is easy to miss patterns that affect long-term progress.
- Tracks long-term client progress: Accurate notes help you monitor behavioral changes and emotional development across multiple sessions.
- Demonstrates intervention effectiveness: Documentation provides evidence for supervisors, insurance companies, and auditors that therapeutic strategies were applied consistently.
- Identifies emerging group dynamics: Notes reveal patterns like repeated conflicts, withdrawal, or dominant behaviors that affect session outcomes.
- Protects professional accountability: Thorough documentation creates a defensible record of clinical decisions, interventions, and client safety considerations.
- Supports therapist self-reflection: Reviewing notes allows you to evaluate which interventions engage clients, foster group cohesion, and need adjustments.
- Prevents missed insights: Without detailed documentation, critical behaviors, client progress, and group trends can be overlooked, compromising treatment quality.
- Ensures continuity of care: Consistent session records allow future therapists or co-facilitators to understand client needs and group dynamics quickly.
Also read: How to Write EMDR Progress Notes Effectively (With Template + Examples)
Common Formats for Writing Group Therapy Notes
Therapists use structured documentation formats to organize group therapy notes clearly and maintain consistent clinical records. Each format focuses on different aspects of the session, such as observable behavior, treatment goals, or therapist interventions.
Choosing the right format helps you document group discussions, client participation, and therapeutic outcomes in a way that supports supervision, treatment planning, and compliance reviews.
| Format | What to document | When therapists typically use it |
| SOAP notes | Document client-reported experiences from the session, observable participation, therapist interpretation of progress, and next treatment steps. Capture both what clients share and what you observe during group interaction. | Therapists commonly use SOAP notes in healthcare and clinical environments where documentation must clearly separate client statements, clinical observations, and treatment planning. |
| DAP notes | Record session data such as client statements, participation in discussions, and group dynamics, followed by the therapist’s clinical assessment and next-session plan. This format combines subjective and objective observations into a single data section. | Therapists choose DAP notes when they need concise documentation that still includes clinical interpretation and clear follow-up planning. |
| GIRP notes | Focus documentation on the specific treatment goal addressed during the session, the interventions used to support that goal, how the client responded, and the next therapeutic steps. | Therapists often use GIRP notes in goal-driven therapy programs where progress toward measurable treatment objectives must be documented regularly. |
| BIRP notes | Document observable client behavior during the session, therapeutic interventions introduced by the therapist, the client’s response to those interventions, and the plan for upcoming sessions. | Therapists typically use BIRP notes in behavioral health settings where documenting behavior change and intervention outcomes is essential. |
Selecting one documentation format and using it consistently helps you maintain structured, clear, and clinically useful group therapy records.
Also read: How to Write ABA SOAP Notes: Best Practices & Examples
Key Components of Effective Group Therapy Notes
A well-structured group therapy note ensures that every session is clearly documented, showing client behavior, participation, and therapeutic interventions. Recording these elements systematically supports treatment planning, supervision, and compliance while helping track progress over time.
| Element | What to Include |
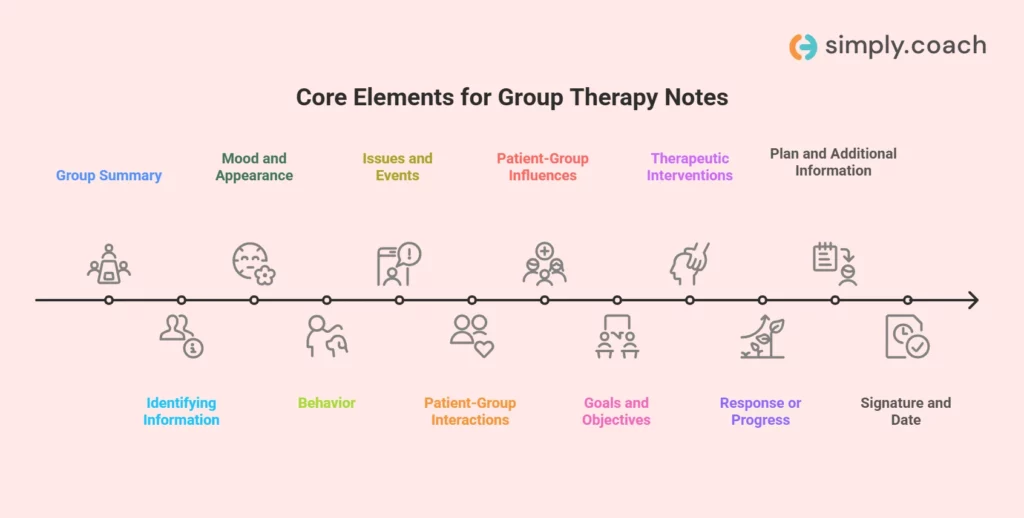
| Group summary | Group name, discussion topic/theme, session date and times, schedule and format, counselor’s name, number of participants, interventions used.Maintain same summary for each client but exclude individual names; use a separate attendance list. |
| Identifying Information | Full name, client ID number, date of birth, organization name, optional details like gender or contact info.Double-check to ensure accuracy and compliance. |
| Mood and appearance | Demeanor (anxious, withdrawn, etc.), facial expressions, general hygiene and appearance, emotional affect.Use a mental status checklist and note changes from prior sessions. |
| Behavior | Participation in exercises/discussions, willingness to share personal experiences, response to peer feedback, body language/nonverbal cues.Note both engagement and challenges to tailor interventions. |
| Issues and events | Conflicts between members, emotional outbursts, interruptions/disengagement, interventions applied.Document factual descriptions of events and therapist responses. |
| Patient-group interactions and reactions | Roles assumed (leader, observer, passive participant), peer reception and inclusion/exclusion, engagement in exercises/discussions.Highlight positive and negative patterns. |
| Patient-group influences | How the client impacts group discussions/mood and how the group impacts the client’s attitudes, decisions, or behavior.Be specific about influence and response. |
| Goals and objectives | Individual treatment goals addressed, objectives targeted by discussion/exercises.Document client participation relative to goals for measurable progress tracking. |
| Therapeutic interventions | Exercises, roleplays, discussions conducted, techniques like cognitive reframing, grounding, or mindfulness.Specify which interventions were used for which clients and why. |
| Response or progress | Behavioral/emotional changes, engagement level, movement toward/away from goals.Record concrete examples of progress or challenges. |
| Plan and additional information | Homework/skill practice, planned interventions/focus areas for next session, anticipated absences or schedule changes.Connect each plan step to treatment goals. |
| Signature and date | Therapist signature and credentials, session date/time, next appointment, supervisor signature if required.Sign immediately after completion for authenticity and compliance. |
Related: How to Set Goals that Help Clients Achieve Progress in Therapy
How to Write Effective Group Therapy Notes
Documenting a group session requires capturing more than individual client behavior. You must record how members interact, how interventions influence the discussion, and how each client progresses toward treatment goals.

Learning how to write group therapy notes effectively helps you produce documentation that accurately reflects the therapeutic process while supporting supervision, treatment planning, and clinical review.
1. Choose the documentation format before writing the note
Group therapy notes should follow a structured clinical format so that observations, interventions, and client responses are documented consistently. Selecting a format before writing prevents missing key clinical details and helps maintain uniform documentation across sessions.
Tips
- Choose a format approved by your organization or clinical supervisor.
- Use the same format for all group sessions to maintain consistency.
- Select a format that clearly separates observations, interventions, and plans.
- Use templates within your EHR or documentation system to speed up note writing.
2. Focus on observable participation rather than general engagement
Group therapy notes should describe exactly how the client participated in the session. Statements such as “client was engaged” do not explain what the client actually contributed to the discussion.
Documenting observable behavior helps you track participation patterns and evaluate whether the client is becoming more comfortable sharing in the group environment.
Tips
- Describe what the client said during discussions.
- Note how frequently the client contributed to group conversations.
- Record whether the client responded to peer feedback or therapist prompts.
- Document participation in exercises, role-plays, or reflection activities.
Example
- Weak documentation: Client participated in group discussion.
- Strong documentation: Client shared two personal experiences related to workplace stress and responded to feedback from three group members.
3. Record how group interactions influence the client’s participation
Group therapy works because clients learn from one another’s experiences. Documenting these interactions helps explain why a client became more open, reflective, or emotionally engaged during the session.
Your notes should show how peer comments, shared experiences, or disagreements influenced the client’s behavior.
Tips
- Document when another member’s story prompts the client to share.
- Note moments when peer support encourages emotional expression.
- Record interactions where the client changes perspective after group discussion.
- Capture situations where group feedback influences the client’s coping strategies.
Example: Client initially remained silent while others discussed workplace conflict. After another member described a similar experience with supervisor criticism, the client began discussing personal concerns about authority figures.
4. Use objective behavioral language instead of interpretations
Clinical documentation should describe what you observe rather than interpreting the client’s intentions or emotions. Subjective descriptions can introduce bias and make the note less reliable.
Objective language focuses on behaviors, communication patterns, and visible emotional responses.
Tips
- Describe posture, tone of voice, and eye contact.
- Document verbal responses rather than emotional assumptions.
- Avoid judgmental words such as lazy, dramatic, or unmotivated.
- Focus on behaviors that can be directly observed during the session.
Example
- Weak documentation: Client seemed uninterested in the discussion.
- Objective documentation: Client remained silent during the discussion, avoided eye contact, and required two prompts before responding to therapist questions.
5. Link group discussion to the client’s treatment goals
Group therapy documentation should clearly show how session discussions support the client’s treatment objectives. Linking observations to treatment goals helps track measurable therapeutic progress.
This connection also allows supervisors or other clinicians to understand why the session content is clinically relevant.
Tips
- Reference the specific treatment goal addressed during the session.
- Document behaviors that show progress toward that goal.
- Explain how the discussion helped the client develop insight or skills.
- Note when the client struggles to apply therapeutic strategies.
Example
- Observation: Client discussed workplace stress triggers during the group conversation.
- Connection to treatment goal: This discussion supports the treatment objective of identifying emotional triggers and developing coping strategies for workplace anxiety.
6. Document the therapeutic interventions used during the session
Group therapy notes should explain which therapeutic strategies were used and how they supported the discussion. Without documenting interventions, it becomes difficult to evaluate whether therapy techniques are effective.
Recording interventions also helps maintain continuity when multiple clinicians facilitate the same group.
Tips
- Identify the therapeutic exercise used during the session.
- Explain the purpose of the intervention.
- Document how group members responded to the activity.
- Record whether the intervention encouraged participation or reflection.
Example: Therapist introduced a cognitive reframing exercise to help members identify negative assumptions about workplace criticism. Clients discussed alternative interpretations of feedback from supervisors.
7. Document meaningful peer interactions and disagreements
Peer feedback often leads to important therapeutic insights. Recording these interactions helps illustrate how the group environment influences client thinking and emotional responses.
Conflicts or disagreements can also provide opportunities for reflection and should be documented when they shape the conversation.
Tips
- Record supportive comments from peers that encourage participation.
- Document disagreements that lead to deeper discussion.
- Note how you guided the group to maintain respectful dialogue.
- Capture insights that emerge from peer feedback.
Example: Client initially disagreed with another member’s coping strategy for handling workplace criticism. After discussion, the client acknowledged experiencing similar feelings of inadequacy when receiving feedback.
8. Track changes in participation or emotional openness during the session
Clients often become more comfortable participating as the session progresses. Observing these changes can reveal improvements in confidence, communication, and emotional expression.
Tracking these patterns across sessions helps therapists evaluate long-term engagement in the group.
Tips
- Compare early-session participation with later discussion.
- Document increased willingness to share personal experiences.
- Record shifts in emotional tone during the session.
- Compare participation with behavior in previous sessions.
Example: Client spoke minimally during the first half of the session but actively participated in the closing discussion on coping strategies and shared one personal example.
9. Write notes immediately after the session
Group therapy sessions involve many interactions and emotional cues that can be difficult to recall later. Writing notes shortly after the session helps preserve the accuracy of your observations.
Developing this habit is essential when learning how to write group therapy notes, especially when documenting multiple clients in a single session.
Tips
- Record brief observations during the session using quick prompts.
- Complete documentation within 15–20 minutes after the session ends.
- Review the note before saving to ensure all key interactions are captured.
- Add missing details while the discussion is still fresh in memory.
Example
Quick post-session capture: Client participated in role-play exercise, received supportive feedback from two peers, and identified two workplace stress triggers during discussion.
These notes can then be expanded into a full clinical record.
Also read: 11 Group Therapy Techniques Every Therapist Should Use in 2026
Group Therapy Notes Examples
Writing group therapy notes becomes more complex because you must document both individual behavior and group interaction. Each note should show how the session topic, therapeutic interventions, and peer responses influence a client’s progress toward treatment goals.
The examples below illustrate how therapists document group sessions using different clinical formats. These examples demonstrate how to structure notes clearly while capturing meaningful participation, behavioral observations, and treatment planning.
| Example 1 – Anxiety Support Group (SOAP Format)Client: Emily R.Date: 03/10/2026Group topic: Managing workplace anxiety triggersNumber of clients attending group: 7Subjective: Emily reported increased anxiety during workplace meetings. She shared that criticism from supervisors often triggers rumination and sleep disturbances.Objective: Emily participated actively in the discussion and described two recent situations where workplace feedback caused emotional distress. She maintained eye contact with group members and responded to peer suggestions about stress management.Assessment: Emily demonstrated improved insight into her anxiety triggers compared to the previous session. Her willingness to discuss workplace stress indicates growing comfort sharing personal experiences within the group.Plan: Next session will focus on cognitive restructuring techniques for workplace anxiety. Emily will track anxiety triggers during the week and note coping strategies used in response. |
| Example 2 – CBT Group Therapy Session (DAP Format)Client: Michael T.Date: 03/11/2026Group topic: Identifying cognitive distortionsNumber of clients attending group: 6Data: The therapist introduced a cognitive restructuring exercise focused on identifying negative automatic thoughts. Michael described feeling discouraged after receiving critical feedback from a coworker. During discussion, he recognized that he often interprets feedback as personal failure rather than constructive guidance. Michael participated in the group worksheet activity and discussed examples of “all-or-nothing thinking.” Two group members shared similar experiences, which encouraged Michael to reflect further on his reactions to criticism.Assessment: Michael demonstrated improved awareness of cognitive distortions affecting his workplace stress. His engagement during peer discussions suggests that group feedback helped him reconsider rigid thinking patterns.Plan: Michael will complete a cognitive thought record during the week to identify negative thinking patterns. The next session will focus on replacing distorted thoughts with balanced interpretations. |
| Example 3 – Addiction Recovery Group (GIRP Format)Client: Daniel K.Date: 03/09/2026Group topic: Relapse prevention strategiesNumber of clients attending group: 8Goal: The session focused on identifying triggers that increase relapse risk and developing strategies to maintain sobriety. Daniel’s treatment plan includes recognizing emotional triggers related to past substance use.Intervention: The therapist facilitated a structured discussion on relapse triggers and coping strategies. Group members shared personal relapse experiences and identified situations that increase cravings. The therapist also introduced a brief grounding exercise to help manage urges.Response: Daniel initially remained quiet during the discussion but later shared that social isolation often precedes cravings. After hearing similar experiences from two other members, he discussed strategies that previously helped him avoid relapse.Plan: Daniel will create a personal trigger list and identify three coping strategies to practice during the week. The next group session will focus on building relapse prevention routines. |
| Example 4 – Anger Management Group (BIRP Format)Client: Jason L.Date: 03/12/2026Group topic: Recognizing early signs of anger escalationNumber of clients attending group: 6Behavior: Jason appeared tense at the beginning of the session and initially avoided contributing to the group discussion. During the group exercise, he described recent conflicts with coworkers and acknowledged difficulty recognizing early signs of frustration.Intervention: The therapist introduced an anger awareness exercise that focused on identifying physical warning signs of escalating anger. Group members practiced describing personal triggers and discussed strategies for interrupting escalation.Response: Jason gradually became more engaged in the discussion and shared that he often notices muscle tension and increased heart rate before reacting during arguments. He responded positively to peer suggestions about using brief time-outs during workplace conflicts.Plan: Jason will track early anger cues during the week and practice using a brief pause technique before responding to conflict situations. The next session will focus on communication strategies for managing disagreements. |
Streamline your documentation and track client progress effortlessly.
Get free SOAP, DAP, GIRP, and BIRP group therapy note templates from Simply.Coach. Streamline your documentation and track client progress effortlessly. Ready-to-use and easy to customize for every session.

Frequent Mistakes Therapists Make When Writing Group Therapy Notes
Group therapy documentation requires careful attention because each note must capture both individual client behavior and group interaction. Avoiding common documentation mistakes helps maintain clear clinical records and ensures your notes accurately reflect therapeutic progress.
- Writing identical notes for every client: Copy-pasting the same note for all participants ignores individual participation and responses. Each note should document how the specific client spoke, interacted with peers, and responded to the intervention.
- Including identifying details about other group members: Mentioning another client’s name or personal information violates confidentiality. Describe interactions generically, such as “another group member shared a similar experience.”
- Failing to link observations to treatment goals: Notes that only describe session activities do not show clinical value. Document how the client’s behavior or discussion relates to their treatment objectives.
- Over-documenting irrelevant session details: Recording minor logistics or casual conversation reduces clarity. Focus on clinically relevant information such as emotional reactions, participation, and intervention outcomes.
- Ignoring group dynamics that influence the client: Group therapy outcomes depend on peer interaction and feedback. Document how the group affected the client’s engagement, insight, or emotional response.
- Using vague or subjective language: Phrases like “client did well” or “seemed upset” lack clinical value. Record observable behaviors such as how often the client spoke, responded to peers, or engaged in exercises.
Consistent, precise documentation allows you to track participation patterns, evaluate intervention effectiveness, and maintain reliable records for supervision, audits, and long-term treatment planning.
Also read: Best Examples & Practices for Writing Counseling Session Notes
Conclusion
Clear and structured group therapy notes are essential for documenting client participation, tracking therapeutic progress, and maintaining reliable clinical records. When your notes capture observable behavior, group interactions, and connections to treatment goals, they become valuable tools for treatment planning, supervision, and long-term client care.
Using structured formats, documenting meaningful observations, and avoiding common mistakes helps ensure your notes remain accurate, consistent, and clinically useful. Incorporating examples and ready-to-use templates can also make documentation faster while maintaining high standards of record-keeping.
How Simply.Coach Can Enhance Your Therapy Practice
Simply.Coach is a secure HIPAA-compliant therapy practice management software designed to help therapists manage sessions, documentation, and client relationships in one place. It simplifies administrative work so you can focus more on client care.
Here’s how it supports your therapy practice:
- Structured note templates: Use customizable SOAP, DAP, BIRP, and GIRP templates to document sessions consistently.
- Customizable note-taking features: Capture session details quickly and consistently.
- Session scheduling: Manage appointments easily with integrated calendars and automated reminders.
- Integrated video sessions: Conduct online therapy sessions using Zoom, Google Meet, or Microsoft Teams integrations.
- Progress tracking: Monitor client development over time using structured records and progress insights.
- Secure client data storage: Maintain HIPAA-compliant cloud storage to protect sensitive client information.
- Centralized client management: Access client profiles, session history, and documentation from a single dashboard.
By combining effective group therapy documentation practices with Simply.Coach, you can streamline your workflow, maintain high-quality records, and focus more on supporting meaningful client progress.
FAQs
1. How to write a therapy group note?
Start with the session basics such as date, topic, facilitator, and number of participants. Then document each client’s participation, observable behavior, peer interactions, and response to therapeutic interventions. Use structured formats like SOAP or DAP to keep the note clear and clinically consistent.
2. What is a short note on group therapy?
A short group therapy note is a brief clinical summary of the session that highlights the discussion topic, key interventions, and the client’s participation. It focuses only on clinically relevant observations and progress toward treatment goals. Concise notes still maintain essential documentation for treatment continuity and compliance.
3. Which is an example of group therapy?
Examples of group therapy include CBT skill-building groups, addiction recovery groups, anxiety support groups, and anger management groups. In these sessions, multiple clients work on shared issues through guided discussions, exercises, and peer feedback facilitated by a therapist.
4. How long should a group therapy note be?
A typical group therapy note is about one page per client, depending on the session content and participation level. Clients who actively contribute may require more detailed documentation than those with minimal engagement. The goal is concise but clinically meaningful documentation.
5. When should therapists write group therapy notes?
Therapists should complete group therapy notes immediately after the session whenever possible. Writing notes soon after the session improves accuracy because details about participation, interactions, and interventions are still fresh. Delayed documentation increases the risk of missing important clinical observations.
6. What should be included in group therapy documentation?
Group therapy documentation should include the session topic, therapist interventions, client participation level, group dynamics, and progress toward treatment goals. It should also capture meaningful interactions between group members and how those interactions influenced the client’s response.