School counselors often balance multiple responsibilities. They support students, coordinate with teachers, communicate with parents, and manage administrative tasks. In the middle of these demands, writing clear and accurate counseling notes can quickly become time-consuming.
Yet documentation remains essential for tracking student progress, maintaining professional accountability, and ensuring continuity of support across sessions.
For counselors working in busy school environments, having a reliable framework for writing counseling notes can simplify documentation while ensuring records remain clear, concise, and professionally appropriate.
Updated for 2026, this guide outlines practical approaches counselors can use to write effective counseling notes, along with structured templates that support consistent documentation.
It explains how to write counseling notes, explore common documentation formats used in school counseling, and share free templates counselors can use to streamline their note-taking process.
Key takeaways
- Counseling notes help maintain continuity across sessions by capturing key themes, interventions, and follow-up plans that guide future support for clients or students.
- Structured formats such as SOAP, DAP, and BIRP make documentation more consistent, helping counselors record essential details without turning notes into lengthy transcripts.
- Effective counseling notes focus on signal rather than detail, documenting observations, client responses, and clinical reasoning instead of recording every part of the conversation.
- Writing notes shortly after sessions improves accuracy, ensuring important insights and behavioral observations are captured while the interaction is still fresh.
- Confidentiality and secure storage are critical, as counseling notes may be reviewed by supervisors, administrators, or legal authorities in certain circumstances.
- Templates, examples, and progress-note frameworks can simplify documentation, especially for counselors managing multiple clients or sessions each week.
- Digital platforms like Simply.Coach help streamline documentation by organizing session notes, goals, and follow-up actions in one place, making it easier to track progress over time.
What Are Counseling Notes (And Why Counselors Need Them)
Counseling notes are professional records that document key elements of a counseling interaction, including the concern discussed, the counselor’s observations, interventions used, and any agreed follow-up actions.
In school settings, these notes serve a practical purpose: they help counselors track patterns across sessions, maintain continuity of support, and document how student concerns are being addressed over time.
However, documentation in school counseling is often confused with other forms of clinical record-keeping. Understanding the differences helps counselors write notes that are appropriate for educational environments rather than psychotherapy settings.
Types of documentation counselors may encounter
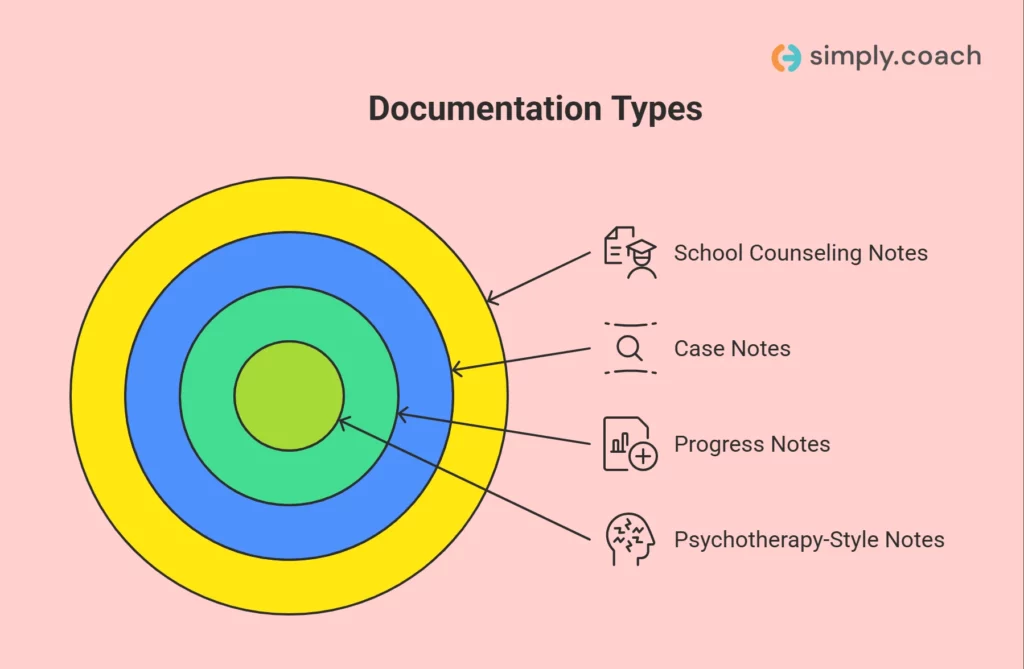
School counselors typically work with several related but distinct forms of documentation:
- School counseling notes: Brief records that summarize the purpose of the meeting, key student concerns, counselor observations, and follow-up actions. These focus on supporting student wellbeing within the school context.
- Case notes: Broader records that track a student’s history of support over time. Case notes may include referrals, parent communication, or coordination with teachers and support staff.
- Progress notes: Structured summaries documenting how a student’s situation evolves across sessions. These often follow formats like SOAP, DAP, or BIRP to track interventions and responses.
- Psychotherapy-style notes: Detailed clinical documentation typically used in therapeutic or medical environments. School counseling documentation is usually more concise and education-focused.
Why documentation matters in school counseling
In practice, counseling notes help support several essential responsibilities within school counseling programs:
- Continuity of care: capturing patterns and insights that inform future sessions.
- Record of intervention: documenting what support strategies were used and why.
- Coordination with school personnel: providing context when collaborating with teachers, administrators, or student services teams.
- Professional accountability: maintaining clear records if decisions or interventions are reviewed later.
- Referral support: documenting concerns when students may require additional services outside the school.
What counseling notes are not
Effective documentation is concise and purposeful. Counseling notes are not transcripts or narrative reports of every conversation detail.
They should avoid:
- recording every word spoken during the session
- including unnecessary personal details unrelated to student wellbeing
- replacing professional judgment with excessive documentation
Instead, well-written counseling notes capture the signals that matter most, including student concerns, counselor observations, interventions used, and next steps.
This allows counselors to stay organized while maintaining clear, confidential, and professionally defensible records.
Also read:Coaching the Growth Mindset: A Mindful Approach to Unlocking Leadership Potential
How to Write Counseling Notes? A Complete Step-by-Step Guide
Effective counseling notes in a school setting serve three core purposes: they document the support provided to the student, help counselors track patterns across sessions, and create a professional record of intervention if decisions are later reviewed by administrators, supervisors, or guardians. The challenge is balancing clarity and accountability without turning documentation into lengthy clinical reports.
In school counseling, notes should remain educationally relevant, concise, and observational rather than diagnostic. Instead of narrating the entire conversation, experienced counselors focus on the signals that matter: the concern presented, the student’s perspective, the counselor’s intervention, and the next step for support.
To illustrate how this works in practice, consider the following realistic scenario.
Example scenario: A seventh-grade student, Alex, is referred by a teacher after repeatedly refusing to present in class and avoiding participation. During the counseling session, Alex reports feeling anxious about speaking in front of peers and fears being judged.
A strong counseling note captures the context, observations, and support strategy rather than retelling the entire conversation.
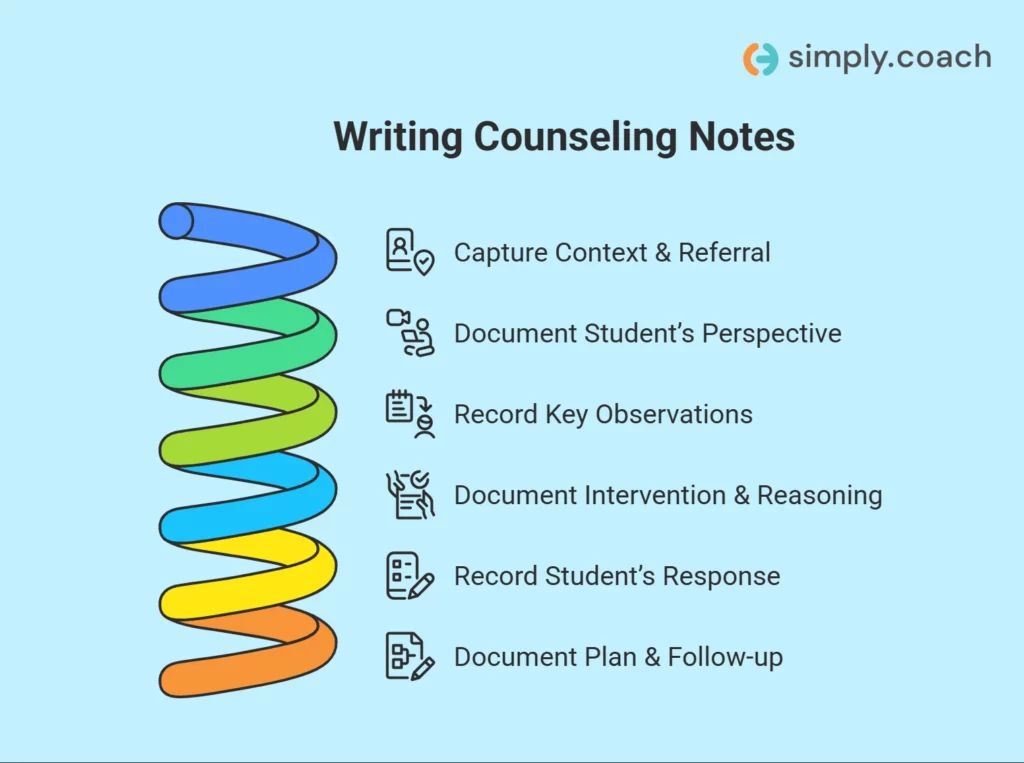
Step 1: Capture context and referral information
The opening section establishes why the session occurred and how the student entered counseling. This context helps future readers understand the purpose of the intervention.
Document:
- student identifier or initials
- grade level
- referral source
- presenting concern
- session type (individual, group, check-in)
Example note entry:
Student: Alex M. (Grade 7)
Referral source: Teacher referral
Session type: Individual counseling
Presenting concern: Avoidance of class presentations and reduced participation in class activities.
School-counseling judgment: Avoid prematurely labeling concerns as clinical diagnoses. In school settings, documentation should remain focused on observable academic or social functioning, not mental-health diagnosis unless formally assessed.
Step 2: Document the student’s perspective
School counseling notes should capture the student’s reported experience in a concise and neutral way. Whenever possible, preserve the student’s language without turning the note into a verbatim transcript.
Example note entry: Student reported feeling “very nervous” before class presentations and worrying that peers might laugh at mistakes. Student described avoiding eye contact with the teacher when presentation assignments are announced.
Why this matters
Recording the student’s perspective helps identify:
- emotional triggers
- cognitive interpretations of events
- avoidance behaviors affecting classroom participation
At the same time, counselors should avoid including excessive personal detail unrelated to the educational context.
Step 3: Record key observations (not just statements)
One of the most valuable elements of counseling documentation is the counselor’s objective observations during the session.
Example observation entry: Student initially spoke quietly and maintained closed body posture during early conversation. Engagement increased after discussing recent classroom experiences.
Best practice for school counselors: Keep a clear distinction between:
- Observation: Student avoided eye contact when describing presentation assignments.
- Inference (avoid stating as fact): Student has severe social anxiety.
School documentation should describe observable behavior, allowing interpretation to remain cautious and context-appropriate.
Step 4: Document the intervention and your clinical reasoning
Counseling notes should briefly record the support strategy used and the reason for choosing it. This demonstrates professional decision-making and continuity of support.
Example note entry: Counselor provided brief guidance on presentation anxiety and discussed strategies such as practicing with a small peer group before presenting to the class. Introduced a simple breathing technique for managing nervousness.
School-specific guidance: Avoid language that appears overly clinical or diagnostic unless working within a therapeutic framework. Notes should remain focused on skills, coping strategies, and academic participation.
Step 5: Record the student’s response to the intervention
An effective note also captures how the student reacted to the intervention. This helps track whether strategies are helpful over time.
Example note entry: Student reported feeling “a little more confident” after discussing practice strategies and agreed to try presenting to a friend before the next class presentation.
Documenting response helps counselors monitor:
- readiness for change
- intervention effectiveness
- engagement with suggested strategies
These signals guide how the next session should unfold.
Step 6: Document the plan and follow-up strategy
The final section outlines next steps in the support process. This keeps the counseling process structured and ensures continuity between sessions.
Document:
- follow-up timeline
- focus for the next session
- coordination with teachers or guardians if relevant
Example note entry: Plan: Follow-up session scheduled in two weeks to review upcoming presentation assignment. Counselor will monitor student’s comfort with practice strategies and reassess participation concerns if avoidance continues.
Example counseling note summary
A concise version of the note might appear as follows:
Session summary: Student referred due to classroom withdrawal and avoidance of presentations. Student reported anxiety related to peer judgment during presentations. Counselor introduced breathing techniques and gradual practice strategies. Student receptive to coping approaches and agreed to attempt presentation practice with a peer. Follow-up session scheduled in two weeks.
Best practices for writing school counseling notes
Over time, experienced counselors develop habits that keep documentation efficient and professionally appropriate.
- Focus on signal, not transcription: capture key insights rather than full conversations.
- Separate observation from interpretation: describe behavior before drawing conclusions.
- Keep documentation educationally relevant: focus on school functioning and student wellbeing.
- Avoid overrecording sensitive information: include only details necessary for professional documentation
- Track patterns across sessions: note progress, recurring concerns, or changes in behavior.
- Protect student confidentiality: avoid unnecessary identifying information.
Many counselors rely on structured documentation formats such as SOAP, DAP, or BIRP to maintain consistency across sessions.
Templates or digital documentation tools can further streamline the process, helping counselors manage records efficiently while maintaining clear and defensible notes.
Counseling Notes for Therapy Sessions: Templates and Examples
Different note formats emphasize different aspects of the counseling process. Some highlight clinical interpretation, others emphasize behavioral change, and some are designed for interdisciplinary communication.
Choosing the right format therefore depends less on preference and more on the type of work being done, the environment you practice in, and how the documentation will be used later.
Below is a practical breakdown of three widely used counseling note structures—DAP, BIRP, and SOAP—along with examples that illustrate how experienced counselors document sessions efficiently while preserving clinical clarity.
DAP notes (data, assessment, plan)
DAP notes are often favored by experienced practitioners because they allow documentation to remain clinically meaningful without becoming overly mechanical.
The structure encourages counselors to capture what occurred, how it was interpreted, and what comes next, while still leaving room for professional judgment. It covers:
Data: Document the client’s statements, behaviors, and relevant session observations. For example, “A client reported increased difficulty sleeping and persistent feelings of overwhelm related to workplace stress. Described rumination about performance expectations and reported reduced motivation outside of work.”
Assessment: Capture the counselor’s clinical interpretation, patterns observed, or emerging themes. For example, “Presentation suggests elevated stress response with cognitive patterns consistent with early depressive rumination. Sleep disruption may be reinforcing fatigue and reduced coping capacity.”
Plan: Outline next steps, interventions, or focus areas for future sessions. For example, “Introduce cognitive restructuring exercises in the next session. Encourage implementation of sleep hygiene strategies and brief evening mindfulness practice. Monitor mood patterns over the next two weeks.”
DAP works particularly well when:
- the session includes complex emotional or cognitive themes
- documentation requires clinical interpretation
- the counselor prefers narrative flexibility within structure
Many practitioners find DAP notes efficient because they emphasize clinical reasoning rather than administrative segmentation.
Download your DAP notes template
Ready to streamline your note-taking process and ensure comprehensive documentation? Download the DAP Notes Template now and simplify your counseling sessions with this efficient format.

BIRP notes (behavior, intervention, response, plan)
BIRP notes are particularly useful when the counselor wants to track how specific interventions influence observable behavior or emotional regulation.
This structure is common in settings where treatment progress must be demonstrated clearly, such as behavioral programs or structured therapeutic environments. It covers:
Behavior: Document observable behaviors, emotional presentation, or reported concerns. For example, “Client presented with visible agitation while discussing workplace conflict. Spoke rapidly and paced intermittently during the session.”
Intervention: Describe the techniques, strategies, or therapeutic methods used. For example, “Counselor guided the client through grounding exercises and facilitated exploration of cognitive triggers contributing to stress escalation.”
Response: Record how the client responded to the intervention. For example, “Client reported feeling calmer after grounding practice and demonstrated increased ability to articulate underlying concerns.”
Plan: Outline follow-up actions or goals for the next session. For example, “Client will practice grounding techniques during periods of heightened stress. Next session will focus on identifying cognitive triggers and introducing reframing strategies.”
BIRP is particularly useful when:
- documenting behavioral change over time
- tracking intervention effectiveness
- working in environments requiring clear treatment accountability
The structure allows counselors to clearly demonstrate the relationship between intervention and client response, which can be valuable in supervision or program evaluation contexts.
Download your BIRP notes template
Ready to efficiently document client behaviors and interventions? Download the BIRP Notes Template now and enhance your session tracking with this organized format.

SOAP notes (subjective, objective, assessment, plan)
SOAP notes remain one of the most widely recognized documentation formats across healthcare and behavioral health disciplines.
Their structure separates client narrative, counselor observations, and clinical interpretation, making them particularly useful in collaborative or multidisciplinary environments. It covers:
Subjective: The client’s self-reported experiences, symptoms, or concerns. For example, “Client reported increased anxiety in social situations following recent workplace changes.”
Objective: Observable behaviors, emotional presentation, or measurable indicators. For example, “Client appeared restless during discussion, avoided eye contact when describing workplace interactions, and spoke rapidly when discussing stressors.”
Assessment: Clinical interpretation of the information gathered. For example, “Symptoms consistent with situational anxiety triggered by recent role changes and increased interpersonal expectations.”
Plan: Recommended interventions, follow-up steps, or treatment adjustments. For example, “Introduce exposure-based coping strategies and mindfulness techniques. Reassess anxiety levels during the next session and adjust treatment approach if symptoms persist.”
SOAP notes are particularly effective when:
- working within integrated care environments
- documentation must be shared with other healthcare professionals
- clarity and standardization are required for insurance or clinical review
Because of their standardized structure, SOAP notes often make cross-disciplinary communication easier.
Download your SOAP notes template
Ready to take your documentation to the next level? Download the SOAP Notes Template today and create structured, easy-to-follow records for each of your sessions. Stay organized and efficient with this time-saving format.

In practice, many experienced counselors develop a preferred structure that aligns with their workflow and clinical approach.
A useful way to think about the formats is:
| Format | Best for |
| DAP | capturing clinical insight and emotional nuance |
| BIRP | tracking interventions and behavioral outcomes |
| SOAP | interdisciplinary documentation and structured records |
The key is not choosing the “correct” format but selecting one that allows documentation to remain clear, efficient, and clinically meaningful.
Over time, the most effective counseling notes become less about the template itself and more about how clearly they capture the evolution of the counseling process.
Confidentiality, FERPA, and Record Access: What You Should Know
One of the most important aspects of counseling documentation in schools is understanding who may legally access those records and under what circumstances.
Unlike private therapy settings, where confidentiality is governed primarily by clinical privacy laws, school counseling records are generally regulated by FERPA (the Family Educational Rights and Privacy Act). This distinction affects how notes should be written, stored, and shared.
For experienced school counselors, documentation is not only about recording sessions, it is about ensuring that records remain professionally appropriate if they are reviewed by parents, administrators, or school officials.
Understanding FERPA in school counseling
FERPA governs access to student educational records in most U.S. schools. In many cases, counseling notes that are stored within the school system may be considered part of the student’s educational record.
This means:
- Parents or legal guardians generally have the right to request access to student records.
- School administrators or authorized personnel may review records when needed for educational support.
- Records must be stored securely and shared only with individuals who have a legitimate educational interest.
Because of this, school counseling notes should always be written with the assumption that they could be reviewed by others within the educational system.
Parent and guardian access to records
Parents sometimes request information about counseling sessions, particularly when concerns about academic performance, behavior, or wellbeing arise. While counselors aim to respect student privacy, FERPA may allow parents to access records that are considered part of the student’s educational file.
In practice, counselors often balance this by:
- documenting educationally relevant information rather than highly personal detail
- focusing notes on observations, concerns, and interventions related to school functioning
- maintaining separate personal reminders or process reflections that are not part of official records
This approach allows counselors to remain transparent while protecting student dignity.
Collaboration with teachers and school staff
School counselors frequently coordinate support with teachers, administrators, and student support teams. In these situations, information sharing should remain purposeful and limited to what supports the student’s educational needs.
For example, counselors might share:
- strategies that help a student participate more comfortably in class
- general information about coping skills or support strategies
- patterns affecting academic engagement
However, personal disclosures made during counseling sessions should not be broadly shared unless necessary for safety or intervention planning.
Legal discoverability of counseling notes
Another factor counselors must consider is that counseling records may become part of legal or administrative reviews in certain situations, such as:
- school investigations
- disciplinary processes
- compliance audits
- legal proceedings involving the student or school
For this reason, professional documentation should remain:
- objective rather than interpretive
- fact-based rather than speculative
- focused on observed behaviors and interventions
Notes written in this way remain clear, professional, and defensible if reviewed later.
How school counseling privacy differs from private practice
Many counseling note templates originate from clinical therapy environments, but school counseling documentation follows a different set of expectations.
Key differences include:
| School Counseling | Private Practice Counseling |
| Governed primarily by FERPA | Governed primarily by HIPAA |
| Records may be accessible to parents | Client records typically remain confidential to the client |
| Documentation focuses on educational impact | Documentation may include deeper clinical interpretation |
| Collaboration with school staff is common | Information sharing is more restricted |
Understanding these distinctions helps counselors document sessions in ways that align with both ethical practice and school policies.
Writing notes with privacy and professional accountability in mind
In practical terms, school counselors often approach documentation with a simple guideline: write notes that are clear, useful, and appropriate if they were read by a parent or administrator.
This means focusing on:
- the student concern or referral context
- the counselor’s observations
- the support strategies discussed
- the next step in the counseling process
When written thoughtfully, counseling notes can support effective student care while maintaining the privacy, professionalism, and legal awareness required in school environments.
How Simply.Coach Helps Counselors Manage Session Documentation
When notes, action items, and session reflections are scattered across notebooks, spreadsheets, or disconnected systems, it becomes harder to review progress or identify patterns in student development.
Simply.Coach, the leading digital coaching platform, helps counselors centralize their documentation and session management in one place. Instead of maintaining separate tools for scheduling, progress tracking, and session notes, the platform allows counselors to manage the entire counseling journey within a single system.
Key features that support structured counseling documentation include:
- Client workspaces → Each client or student has a dedicated workspace where counselors can record session notes, track goals, share resources, and review progress across sessions. Clients can also view goals, track progress, and add their own reflections within the workspace.
- Goal and progress tracking → Counselors can define goals and monitor progress over time, helping ensure that counseling sessions remain outcome-focused rather than isolated conversations.
- Action plans → Counselors can convert insights from a session into clear action steps and track whether those actions are completed between sessions, helping clients stay accountable to their goals.
- Forms and reflection tools → Built-in forms and questionnaires allow counselors to gather reflections, assessments, or feedback before or after sessions, helping generate structured insights that inform counseling notes.
- Integrated scheduling → Scheduling tools sync with calendars and help manage session bookings, reminders, and reschedules from one place.
- Session and engagement management → The platform helps professionals manage one-to-one, team, or group engagements while keeping all session records and progress data organized.
By keeping session notes, goals, reflections, and action plans connected within a single system, Simply.Coach helps counselors maintain structured, easy-to-review documentation.
Conclusion
Middle school group counseling activities help students build essential social and emotional skills during a critical stage of development. Through structured discussions and interactive exercises, students can practice communication, empathy, problem-solving, and emotional awareness in a supportive peer environment. Over time, these experiences strengthen confidence, improve relationships, and help students navigate everyday challenges more effectively.
At the same time, running effective group programs requires consistent planning, documentation, and follow-through across sessions. Platforms like Simply.Coach, the leading digital coaching platform, help counselors keep session plans, notes, and progress insights organized in one place—making it easier to manage counseling programs while focusing on meaningful student engagement.
See how Simply.Coach fits your practice.
FAQs
1. How long should counseling notes be?
Counseling notes should be concise but complete enough to document the key elements of a session. Most professionals aim for brief summaries that capture the main concerns, interventions, and next steps, rather than detailed transcripts. The goal is to record information that will still be meaningful when reviewing the case weeks or months later.
2. Can counseling notes be shared with other professionals?
Counseling notes may be shared with other professionals involved in a client’s care when appropriate and permitted by institutional policies or consent agreements. In collaborative settings such as schools or healthcare systems, summaries from session notes may help teachers, administrators, or healthcare providers coordinate support while respecting confidentiality guidelines.
3. How should counseling notes be stored securely?
Counseling notes should be stored in secure and confidential systems that limit access to authorized individuals. Many organizations use encrypted digital platforms or protected record systems to ensure compliance with privacy standards. Physical notes should also be stored in locked cabinets or restricted-access locations.
4. What is a therapy progress notes cheat sheet?
A therapy progress notes cheat sheet is a quick reference guide that summarizes key documentation elements counselors should include in session notes. These guides often outline common note structures, reminders for objective language, and prompts that help professionals capture important session insights efficiently.
5. Are counseling notes ever used in legal situations?
Yes. In some circumstances, counseling notes may be reviewed in legal or administrative contexts, such as school investigations, compliance audits, or court proceedings. For this reason, counselors are encouraged to write notes that are clear, factual, and professionally objective, assuming they may eventually be read by others.
6. Are counseling notes written during or after a session?
Many counselors prefer writing notes immediately after the session ends. This approach allows the counselor to remain fully present with the client during the conversation while still capturing details accurately while the session is fresh in memory.
7. What makes counseling notes clinically useful over time?
Counseling notes become most useful when they help counselors identify patterns across sessions. Notes that track recurring concerns, behavioral changes, intervention responses, and follow-up plans allow professionals to monitor long-term progress and adjust their counseling approach accordingly.